Archives for Healthcare (page 1 / 5)
February 17, 2014 11:49 AM CST
By Joe Martin in Healthcare
Interesting.
One of the largest and most meticulous studies of mammography ever done, involving 90,000 women and lasting a quarter-century, has added powerful new doubts about the value of the screening test for women of any age.
It found that the death rates from breast cancer and from all causes were the same in women who got mammograms and those who did not. And the screening had harms: One in five cancers found with mammography and treated was not a threat to the womans health and did not need treatment such as chemotherapy, surgery or radiation.
… an editorial accompanying the new study said that earlier studies that found mammograms helped women were done before the routine use of drugs like tamoxifen that sharply reduced the breast cancer death rate. In addition, many studies did not use the gold-standard methods of the clinical trial, randomly assigning women to be screened or not, noted the editorial’s author, Dr. Mette Kalager, and other experts.
Dr. Kalager, an epidemiologist and screening researcher at the University of Oslo and the Harvard School of Public Health, said there was a reason the results were unlike those of earlier studies. With better treatments, like tamoxifen, it was less important to find cancers early. Also, she said, women in the Canadian study were aware of breast cancer and its dangers, unlike women in earlier studies who were more likely to ignore lumps.
“It might be possible that mammography screening would work if you don’t have any awareness of the disease,” she said.
∞
November 13, 2013 07:53 AM CST
By Joe Martin in Healthcare
Do Americans really pay more for healthcare and get less for it than most other industrialized countries? Avid Roy does some myth busting.
If you really want to measure health outcomes, the best way to do it is at the point of medical intervention. If you have a heart attack, how long do you live in the U.S. vs. another country? If you’re diagnosed with breast cancer? In 2008, a group of investigators conducted a worldwide study of cancer survival rates, called CONCORD. They looked at 5-year survival rates for breast cancer, colon and rectal cancer, and prostate cancer. I compiled their data for the U.S., Canada, Australia, Japan, and western Europe. Guess who came out number one?
∞
April 08, 2013 03:53 PM CDT
By Joe Martin in Healthcare
Dr. Pauline Chen, writing at the New York Times.
The researchers then compared these outcomes to those of patients who were not covered by Medicare and therefore not restricted to having their operations done at centers of excellence. Even after adjusting for individual patient risk factors and the specific type of bariatric procedure performed, they found no differences in complication rates or outcomes between Medicare and non-Medicare patients. Moreover, they discovered that many of the improvements had been under way prior to 2006.
In other words, the much-heralded policy of funneling patients to centers of excellence has had little effect on how patients do.
Over the past several years, I've seen lots of people talking about how this or that government program fixed this or that problem in the United States. And, almost invariably, I'll see economists pointing out that the trend line was already declining before the government got involved and that the government's involvement did nothing to speed up the change.
Without this research, this Medicare policy would have received the same praise even though it, too, deserves none of the credit.
∞
April 04, 2013 09:49 AM CDT
By Joe Martin in Healthcare
From Dr. Elizabeth Dzeng, at The Health Care Blog:
The social worker informed him that Medicare would not pay for home care nurse visits or supplies. BUT, Medicare pays for inpatient rehabilitation, which he would be eligible for to receive these antibiotics. Given the choice of paying $7000 for home administration versus $0 for inpatient rehabilitation, naturally he chose inpatient rehabilitation.
The problem is, is that his inpatient stay costs taxpayers approximately $21,000. $350 for room and board plus additional costs for antibiotics and supplies, totaling approximately $500 a day. Furthermore, although he was well enough to be discharged home before Christmas, he needed to stay until he could be placed in rehab. Because of holiday scheduling, most rehabilitation facilities were not accepting admissions. Thus, he had to stay in the hospital an extra four days in the hospital over the weekend and holidays. Given that the average cost of a hospital stay is $2338 in Maryland that added an additional $9352 or so of unnecessary expenses.
In sum, because financial incentives encouraged my patient to spend $0 rather than $7000 out of pocket, Medicare spent an unnecessary added $30,000 on his hospitalization and care.
This is the problem with third party payment. When someone else is paying for your medical care, you have to follow their rules. And their rules will often force you to make dumber decisions than you would make if you were spending your own money.
∞
April 04, 2013 07:11 AM CDT
By Joe Martin in Healthcare
Gautam Naik, writing for the Wall Street Journal:
Inside a warren of rooms buried in the basement of Gregorio Marañón hospital here, Dr. Aviles and his team are at the sharpest edge of the bioengineering revolution that has turned the science-fiction dream of building replacement parts for the human body into a reality.
Now, with the quest to build a heart, researchers are tackling the most complex organ yet. The payoff could be huge, both medically and financially, because so many people around the world are afflicted with heart disease. Researchers see a multi-billion-dollar market developing for heart parts that could repair diseased hearts and clogged arteries.
Lab grown replacement organs using adult stem cells. Awesome. I see no reason to back down from my prediction that my generation will have a substantially longer lifespan than my grandparents' generation.
∞
March 13, 2013 12:01 PM CDT
By Joe Martin in Healthcare
Here's something interesting from my files.
Medical personnel are fond of saying that you can't practice medicine like a business. They often believe that their work is unique and can't be easily optimized by industrial engineers. But there is some room for improvement. Take scheduling. What if you did today's work today? Worry about next week, next week. Don't try to schedule it today.
A few doctors have started applying that principle in their offices and have found that their patients spend less time in their waiting rooms and spend less time waiting for an available appointment. And the doctors spend less time being overbooked and overworked. The concept is called "open access scheduling" and allows doctors to leave most of their time unbooked.
[P]atients start calling at 9 a.m. and are assigned 15-minute time slots on a first-call, first-serve basis. Those who want a traditional scheduled appointment can try for the two to three hours a day he reserves for advanced bookings, usually for annual physicals or patients who need regular follow-ups. A few extra slots are left open for walk-ins or emergencies.
This is the type of innovation and experimentation that you'd see more of, if patients paid for their care directly, giving them the freedom to shop around and consult different doctors. That kind of open ended market would also give providers more freedom to experiment with how they practice healthcare, rather than being tied to the rules of large HMOs and large group practices.
∞
March 12, 2013 08:33 AM CDT
By Joe Martin in Healthcare
Americans in urban areas think of dental services as a kind of regular maintenance. It's little different than changing the oil in your car and occurs about as often. But that's not true for everyone.
According to the Pew Center on the States, more than 40 million Americans reside in areas with a shortage of dentists. And individuals without dental health access often end up in the emergency room, which is more expensive for everyone.
Advocacy groups and some state legislators think an alternative type of dental provider, often called a dental therapist, can fill the void. Dental therapists don’t receive as much training as a dentist. But they can perform some of the same basic services — such as pulling teeth and filling cavities — under the supervision of a dentist.
In Minnesota and Alaska, the two states that have practicing dental therapists so far, some of the therapists are able to take their work on the road, traveling to rural areas to treat those who have little or no access to dentists — or who have limited dental coverage. The dental therapists charge less than dentists and are able to take all types of insurance, including Medicaid and Medicare.
“The bottom line is that it will cost a state significantly less to hire dental therapists to provide basic restorative care to the underserved,” said Julie Stitzel, manager for the Pew Children’s Dental Campaign.
How are America's dentists responding to this? Not well.
“The No. 1 obstacle has been organized dentistry,” Pew’s Stitzel said.
“What we’re opposed to is the delegation of surgical procedures,” Faiella said. “Everyone deserves the treatment of a dentist and the care of a dentist.”
He says ADA is developing a range of programs to address the gap — pushing prevention measures such as fluoride and dental sealants, emergency room diversion programs in which dentists partner with community health clinics to ensure people needing dental care don’t end up in the emergency department — and an ad campaign to encourage parents to make sure their kids brush twice a day.
An ad campaign. That'll certainly take care of the dental problems of America's rural population. After all, they deserve a dentist not a less personage. And if they can't have a dentist? They're better off having nothing.
∞
October 30, 2012 03:27 PM CDT
By Joe Martin in Healthcare
John Cochrane recently wrote about healthcare reform. This is the direction we need to go in, not Obamacare.
First, he talked about the insurance side of health care.
To summarize briefly, health insurance should and can be individual, portable, life-long, guaranteed-renewable, transferrable, competitive, and lightly regulated, mostly to ensure that companies keep their contractual promises. “Guaranteed renewable” means that your premiums do not increase and you can’t be dropped if you get sick. “Transferable” gives you the right to change insurance companies, increasing competition.
Insurance should be insurance, not a payment plan for routine expenses. It should protect overall wealth from large shocks, leaving as many marginal decisions unaltered as possible.
Preexisting conditions, lack of insurance by the young and healthy, and spiraling insurance costs– the main problems motivating the ACA -- are neatly addressed by this alternative. Why do we not have a system? Because law and regulation prevent it from emerging. Before ACA, the elephant in the room was the tax deduction and regulatory pressure for employer-based group plans. This distortion killed the long-term individual market and thus directly caused the pre-existing conditions mess. Anyone who might get a job in the future will not buy long-term insurance. Mandated coverage, tax deductibility of regular expenses if cloaked as “insurance,” prohibition of full rating, barriers to insurance across state lines – why buy long term insurance if you might move? – and a string of other regulations did the rest. Now, the ACA is the whale in the room: The kind of private health insurance I described is simply and explicitly illegal.
He finished by writing about the supply of health care and why we have expensive, low quality options.
So, where are the Walmarts and Southwest Airlines of health care? They are missing, and for a rather obvious reason: regulation and legal impediments.
A small example: In Illinois as in 35 other states7, every new hospital, or even major purchase, requires a “certificate of need.” This certificate is issued by our “hospital equalization board,” appointed by the governor (insert joke here) and regularly in the newspapers for various scandals. The board has an explicit mandate to defend the profitability of existing hospitals. It holds hearings at which they can complain that a new entrant would hurt their bottom line.
Specialized practices that deliver single kinds of service or targeted groups of customers cheaply face additional hurdles, as they undermine the cross-subsidization provided by “full service” hospitals. For example, the Institute for Justice is bringing a major suit8 by a specialty colonoscopy practice in Virginia, which local “full service” hospitals managed to ban.
... The increasing spread of medical tourism to cash-only offshore hospitals is a revealing trend. Why does this have to occur offshore? What’s different about the hospital location? Answer: the regulatory regime.
So, what’s the biggest thing we could do to “bend the cost curve,” as well as finally tackle the ridiculous inefficiency and consequent low quality of health-care delivery? Look for every limit on supply of health care services, especially entry by new companies, and get rid of it.
∞
October 30, 2012 01:46 PM CDT
By Joe Martin in Healthcare
John Goodman talks about why Obamacare was flawed from the very beginning.
Do you remember the debates over the Affordable Care Act, aka ObamaCare? Now that repeal of the law has become a major campaign issue, it may be helpful to remember why Congress passed it in the first place.
Early in 2010, as the climactic votes neared, a parade of the legislation's defenders—from the House, Senate and Obama administration—appeared across the media. All had the same message: pre-existing conditions. They named the names of families "victimized" by companies that had refused to sell them insurance, had canceled their coverage or had refused to pay their medical bills.
The message surely resonated, but how many people have actually been affected since the law passed? The Affordable Care Act established a federally funded risk pool—the Pre-Existing Condition Insurance Plan—that allows individuals with such disqualifying conditions to buy a policy for the same premium a healthy person would pay. About 82,000 people have signed up as of July 31, according to the Kaiser Family Foundation's statehealthfacts.org.
That is not a misprint. Out of a population of more than 300 million, some 82,000 have the problem that was cited as the principal reason for spending $1.8 trillion over the next 10 years and in the process turning the entire health-care system upside down.
There is a much better way to ensure people with pre-existing conditions and you don't have to federalize health care in order to do it.
∞
October 30, 2012 12:00 PM CDT
By Joe Martin in Healthcare
Specialization in cancer care could lead to better outcomes at the same price. Instead of having every hospital perform every procedure, it might be better to have hospitals specialize in different procedures.
“If all patients needing surgery for colon cancer were referred to hospitals that have consistently achieved mortality rates in the bottom half of all hospitals performing this operation, then the average mortality rate could fall from a rate of 3.8 percent to 2.4 percent,” Ho said. “And if all patients who require surgical resection for pancreatic cancer were referred to hospitals performing 11 or more of these operations per year, mortality rates could fall by half, from a rate of 6 percent to 3 percent.”
“We were concerned that the centralization of cancer care that would result from referring patients to a smaller set of higher-volume hospitals could give these hospitals additional market power to raise prices,” Ho said. “We also wondered whether higher-volume hospitals might have a different cost structure that would raise or lower costs per patient. We found no statistical evidence that hospitals that performed more of these cancer operations were able to charge higher prices to patients for these services. We found that costs per patient were indeed higher for hospitals performing more pancreatic cancer surgery. However, these higher costs were not passed on to patients as higher prices for patient care.”
∞
October 24, 2012 01:35 PM CDT
By Joe Martin in Healthcare
More ways to communicate with patients that we used to think were brain dead.
Scientists have been able to reach into the mind of a brain-damaged man and communicate with his thoughts.
The research, carried out in the UK and Belgium, involved a new brain scanning method.
Awareness was detected in three other patients previously diagnosed as being in a vegetative state.
The study in the New England Journal of Medicine shows that scans can detect signs of awareness in patients thought to be closed off from the world.
∞
October 24, 2012 10:50 AM CDT
By Joe Martin in Healthcare
It may turn out that fewer patients are actually in a vegetative state than we think.
Researchers are currently testing the Halifax Consciousness Scanner, a device that uses words and tones to measure brain function in patients that have suffered severe trauma or stroke-induced brain injuries.
... In developing the scanner, doctors first measure brain-wave patterns to create a picture of a healthy individual’s brain, which is then compared to the picture that is produced by an impaired brain.
Doctors are then able to determine the extent of the injuries and a long-term outlook for a patient’s recovery.
The team behind the Halifax Consciousness Scanner is hoping to test the device on more brain trauma patients and eventually have units in ambulances and emergency rooms to gain accurate brain status readings of unconscious and semi-conscious patients.
Researchers are also teaming with engineers to develop a hand-held consciousness scanner and headset.
∞
October 23, 2012 02:38 PM CDT
By Joe Martin in Healthcare
Competition is coming to the healthcare system. It's coming very slowly, but it is coming.
In Priceless, I hazarded a guess that employers could cut the cost of hospital care in half by engaging in medical tourism. It’s a variation on what is sometimes called “value-based purchasing” or “reference pricing.” In its pure form, the employer picks a low-cost, high quality facility and covers all costs there. If the employee chooses another hospital, the employee must pay the full extra cost of the more expensive choice. In Priceless, I argued that to take full advantage of the opportunities available, the patients must be willing to travel.
Several large companies are already trying the idea out. As Jim Landers explains:
Wal-Mart Stores Inc., the nation’s largest employer, will jump into medical tourism next year by offering insured employees no-cost heart and spine surgeries at Scott & White Memorial [in Temple, Texas] and seven other hospitals across the country…By using a hospital in the new narrow network, patients could save as much as $5,000 or more…
The hospitals in Wal-Mart’s network — including the Cleveland Clinic and Geisinger Medical Center in Danville, Pa. — have gained national reputations for both quality and value. Physicians and surgeons work under financial incentives rewarding improved patient outcomes.
∞
October 23, 2012 12:34 PM CDT
By Joe Martin in Healthcare
Many politicians were motivated to push for Obamacare because of how much money we're spending on emergency room care, for patients who don't have insurance.
Health care delivered in the emergency room is often derided as expensive and inefficient, the source of our health spending woes. Physician Robert O’Connor has a different way to describe emergency medicine: An incredibly good deal.
O’Connor chairs the department of emergency medicine at the University of Virginia School of Medicine. As an emergency room doctor, he is not unbiased in defending the work he and his colleagues do. He’s also pretty tired of all the rhetoric about emergency rooms as the health spending culprit.
He says that ERs only account for 2 percent of all health care spending—and argues that patients actually get tons of bang for their buck.
... Another surprising data point: Emergency room spending is pretty uniform across different types of insurance coverage. That challenges some of the assumptions that the uninsured tend to visit the emergency room the most frequently. As it turns out, 89 percent of emergency room patients have some form of public or private insurance.
How much government regulation should we do, if we're concerned about 2-4% of overall healthcare spending?
∞
This entry was not tagged.
October 23, 2012 10:29 AM CDT
By Joe Martin in Healthcare
The Congressional Budget Office has estimated ObamaCare will "reduce the amount of labor used in the economy by roughly half a percent" — about 800,000 full-time jobs. It seems likely that four especially steep cliffs — including two where marginal tax rates can approach 100% or more — will factor into work and hiring decisions.
The 50th employee: For companies with 49 workers that do not offer its employees health coverage, the hiring of just one more worker would carry a penalty of $40,000.
The low-income cliff: At 200% of the poverty level is a dividing line. Deductibles for married couples on one side may be $300 vs. $3,500 on the other, according to one estimate provided to the Kaiser Family Foundation by Towers Watson.
The moderate-income cliff: The cliff is even steeper for families at 400% of poverty. Just past that point, families would lose eligibility for ObamaCare subsidies, which can get quite valuable for older workers.
Older workers' cliff: Lastly, consider a 62-year-old worker with $38,500 in income, $4,000 from investments. Such a worker could qualify for a $6,500 ObamaCare subsidy, paying $3,700 toward premiums with perhaps a $2,000 deductible.
But if she retires and claims Social Security, with roughly $14,000 a year in benefits, her ObamaCare premium subsidy would rise to $9,400 with almost no deductible.
Factoring in a state and federal tax bill of $6,500, that worker would have an after-tax, after health cost (premium and deductible) income of $26,000, vs. $17,100 in the old early-retirement scenario. In other words, the pre-tax gap between working and retiring early would shrink from $20,500 to just $8,900.
∞
October 23, 2012 08:00 AM CDT
By Joe Martin in Healthcare
The National Federation of Independent Business (NFIB) published a breakdown of the coming changes to healthcare, due to Obamacare.
Employees will pay a long list of new taxes, some of them hidden. ... Drug companies will pay a new tax on brand-name prescription drugs, but the tax will be passed along to you through higher premiums.
Medical device manufacturers will pay a new 2.3% tax on their products but will pass the tax on to you through higher premiums. One industry analysis suggests this may cause a loss of more than 43,000 jobs. Medical devices range from bedpans to MRI machines.
Employees will lose choices. If your income and family size qualify you for Medicaid, PPACA won’t allow you to stay on your employer’s plan. Example: A couple with 3 children and income of $41,000 can get private insurance through an employer. If the couple has a fourth child, however, PPACA will force them to leave the employer’s insurance and go on Medicaid because the federal poverty level (FPL), which determines who is and is not on Medicaid, increases with family size.
If your household income tends to fluctuate, you may have to move back and forth between a private insurance policy and Medicaid – possibly multiple times per year. Each time this happens, you may have to change doctors, hospital, etc.
∞
October 19, 2012 11:52 AM CDT
By Joe Martin in Healthcare
While urgent care centers typically offer hundreds of medical services, they do not perform surgery and are not equipped to deal with life-threatening emergencies. In most cases, a doctor is on site, although care may be provided by a nurse or physician assistant who is also on staff. Many centers are busiest in the evenings and on weekends, when most doctors' offices are closed.
In the past, at least some of the patients who now go to urgent care centers would have ended up in hospital emergency rooms. While the typical $100 visit to a center is comparable in price to a visit to a doctor's office, an emergency room visit can cost more than twice as much. A 2010 Rand Corp. study found that almost one in five visits to hospital emergency rooms could be treated at urgent care centers, potentially saving $4.4 billion annually in health-care costs.
Better customer service (because of late hours and quick appointments) and lower price. What's not to like? I think the increase in urgent care centers is a very good thing for American healthcare.
∞
October 08, 2012 05:50 PM CDT
By Joe Martin in Healthcare
This is very interesting.
And on Wednesday in Washington DC, Soon-Shiong and his L.A.-based NantHealth will unveil a joint venture with Verizon, Intel, Blue Shield of California and others to create a nationwide system for doctors to share DNA and other data on cancer patients. It will enable doctors to do genetic analysis of a patient's tumor in less than a minute -- a job that now can take from eight to 10 weeks.
"This is something the federal government should have done, but we waited and waited for them," Soon-Shiong told Reuters in an interview.
"It's unconscionable that cancer patients get the wrong diagnosis 30 percent of the time and that it takes so long to treat them with appropriate drugs for their cancer."
Soon-Shiong emigrated to the United States more than three decades ago with his wife Michele Chan, an actress who had a starring role in 80's show "Danger Bay" that aired on CBS and the Disney Channel and guest roles on " MacGyver." Since then, he has methodically climbed the ladder of success by adroitly mixing science and business.
He created drugs to fight diabetes and breast cancer and then sold the companies that produced them for a combined $8.6 billion.
In the four years since selling those companies, he quietly spent more than $400 million of his own money to build a national fiber optic network that would link cancer clinics throughout the country -- the groundwork for the health superhighway.
∞
September 30, 2012 10:53 AM CDT
By Joe Martin in Healthcare
Personalized medicine is the future. It is where the science is going. It is where the technology is going. It is where doctors and patients will want to go. Yet unfortunately for many of us, this is not where the Obama administration wants to go.
John Goodman gives several examples of how personalized medicine has saved lives and improved health. This truly is exciting, cutting edge stuff. But it's not where the government wants to steer the healthcare industry.
ObamaCare's premise rests on the idea that everyone can be given the exact same treatments and medicine can be standardized in order to cut costs. So, it has no provisions for personalized medicine.
∞
April 19, 2012 04:35 PM CDT
By Joe Martin in Healthcare
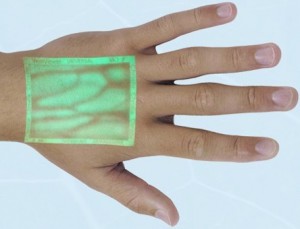
This is a super cool piece of technology.
The instrument uses a near-infrared light that penetrates just below the skin and reflects off blood vessels. VeinViewer senses hemoglobin, the oxygen-carrying component in blood, which an onboard computer uses to distinguish veins from arteries. It then projects an image of veins on the skin surface in a green light.
It's especially useful on dark-skinned patients, whose blue veins aren't readily visible, and overweight patients, whose veins tend to be deeper. It also highlights the tiny veins of infants.
"It's a great tool to reduce a baby's stress," Ginny Johnson, director of women's services at North Hills, said as she demonstrated the instrument on 1-day-old Zoey White. Helped by a little rubbing of her wrist, VeinViewer traced Zoey's threadlike veins as she awoke from a nap.
It costs $17,000 but the patient satisfaction with these things has to be off the charts. If I was spending my own money on healthcare, this would definitely be something that I'd be looking for in the hospital or doctor's office.
∞
